
Osteoarthritis is the commonest form of arthritis with ‘Osteo’ meaning bone and ‘arthritis’ meaning joint inflammation. It is basically a chronic degenerative disorder of the weight bearing joints commonly affecting more women than men. It generally affects the population of age above 45 years but may affect the young also. It is commoner in women above the age of 50 due to menopause.
The disease generally starts with severe pain in a joint on activity and exertion and there might be occasional joint swelling too. It then progresses to pain in joints even while resting. There is morning stiffness but lasts lesser than 30 minutes. Stiffness on initial movement after being immobile for long durations is also complained of. The disease is relentless and generally spreads to other joints in due course of time depending on the presence of various aggravating factors. The commonest joints involved are the knees, hips, finger joints, shoulders and spine. Atypical joint involvement like elbow can be correlated with precious history of trauma.
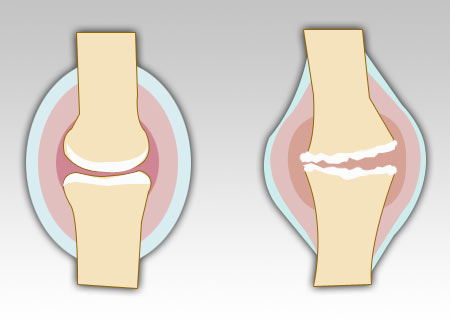
Heberden’s and Bouchard’s nodes may be visible in moderately advanced disease on the finger joints. Deformities like Knock-knees or Bow-legs might develop in advanced disease due to loss of joint space in various compartments of the knees. It is important to differentiate osteoarthritis from other chronic joint disorders like rheumatoid arthritis, gout and more. Investigations like x-ray of the affected joint maybe done to confirm the diagnosis. Subchondral cysts, joint space narrowing, osteophytes (i.e. bony overgrowths) and subchondral bone sclerosis are visible in variable degrees on the x-rays. Other investigations are not required and will not lead to diagnostic confirmation of osteoarthritis presence but helps in ruling out other inflammatory diseases which mimic it. Liver function and blood count may be assessed prior to starting analgesics.
Prognosis depends on how mobile you keep the joints and other factors. These include previous trauma to the joint, obesity, family history of OA, underlying diseases of bone, underlying neuropathic disorder, Concomitant Orthopedic disorder, excessive wear and tear due to overuse and inherited metabolic disorder. Conventional line of treatment involves administration of analgesics to relieve pain and topical counter-irritants for soothing effect. Intra-articular corticosteroid injections are given to reduce inflammation especially in cases of joint effusion. Dietary supplements like glucosamine sulphates have gained recent popularity as effective reducers of the breakdown process in osteoarthritis.
Exercises and weight management form a very integral part in management of osteoarthritis due to its chronic nature and no definite cure. Exercises stretch various muscles involved in the movement of the joint and thus by utilizing these muscles they may be strengthened. Once the muscles around a particular joint are strengthened by exercise they provide stability during everyday movement, help reduce the pain, slow down the degenerative processes.
The following 8 exercises mobilize various groups of muscles around the joints which are commonly affected in osteoarthritis mainly the knee, ankle and hips.
Knee Stretch – Lie on your back with one leg completely outstretched and the other leg bent at the knee. Put a rolled towel under your knee and clasp your hands around your ankle. If you can’t reach the ankle, you can use a belt around the ankle. Pull the ankle towards your bottom and hold for 5 seconds. Repeat 3 times and repeat with towel rolled under the other leg.
Leg-Straightening – Sit on a chair, with the leg to be exercised stretched out in front of you and the heel supported on another table or chair of the same height. Let your leg straighten in this position. Hold there for 30 seconds and repeat with the other leg.
Sit and Stand – Sit with your arms crossed on a chair. Stand up and sit down slowly on a chair. Repeat 10 times. This exercise can be made easier and more difficult by adjusting the height of the chair.
Stepping – Stand in front of a 20 cm high step/stool. Step up 5 times with one leg leading and then repeat with the other leg leading. Repeat 5 times and then repeat with other leg.
Leg-Lift – Sit with your legs out straight and a support behind your back. Place a rolled towel/wedge under your knee. Bend your ankle, straighten the knee and push it down against the towel. Then lift your leg 1 cm off the roll. Return to starting position. Repeat 10 times. Repeat with other leg.
Leg-Weights – Stand with support like the back of a chair. Put a 2kg weight around the ankle. Bend the leg at the knee and lift your foot off the floor. Hold for 10 seconds. Repeat 10 times. Repeat with the weight around the other ankle.
Knee-Squeeze – Stand with support and squeeze a wedge/towel roll between the knees. Keep squeezing while gently bending the knees by 45 degrees. Return to standing position again. Repeat 10 times.
Knee-Lift – Stand on one leg with the knee slightly bent. Lift the other foot off the floor. Hold for 30 seconds or as long as comfortable. Try not to hold onto any support while standing.
Thus by effecting weight loss, using pharmacotherapy and regularly exercising, osteoarthritis can be controlled effectively. It can be managed with minimum pain and discomfort to the patient providing maximum mobility in everyday activities.
– Dr Rachita Narsaria